Keywords: Audace Pharma, Audace Vietnam, Chronic Liver Disease, Chronic Hepatitis, Liver Fibrosis, Liver Symptoms, Hepatitis Etiology, Metavir Stages, Diet for Liver Patients, Liver Function Tests, Chronic Liver Treatment, Hepatocellular Carcinoma (HCC), Liver Fibroscan, ALT AST Levels, Specialized Hepatology Care, Cirrhosis Prevention.
1. Definition and Biological Nature of Chronic Liver Disease
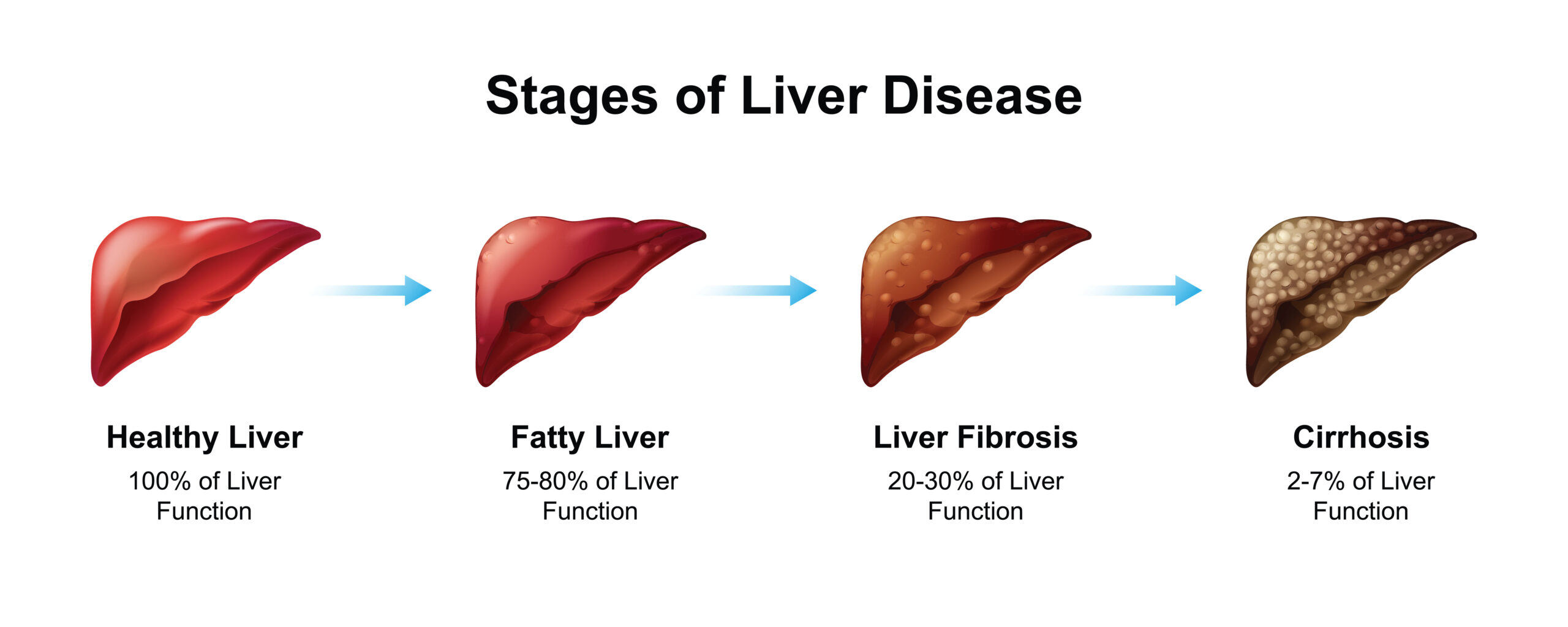
Chronic liver disease is a prolonged pathological process in which the liver parenchyma is continuously or repeatedly injured for at least six months. Biologically, this is the consequence of an imbalance between hepatocyte destruction and the body’s regenerative capacity. When pathogenic factors persist, the liver cannot complete its normal self-healing cycle; instead, it triggers systemic inflammatory responses. Immune cells, such as macrophages and lymphocytes, aggregate in the hepatic lobules, releasing pro-inflammatory cytokines, which alter the liver’s microenvironment and lay the foundation for permanent structural changes in the future.
2. Causes of Liver Disease:
2.1. Etiology of Fibrosis and Parenchymal Structural Transformation
Fibrosis is the most critical hallmark of chronic liver disease. Under physiological conditions, stellate cells reside in the Space of Disse in a quiescent state, storing Vitamin A. However, under the influence of prolonged inflammatory responses, these cells are activated and undergo a phenotypic transformation into myofibroblasts. They begin to produce excessive amounts of extracellular matrix, primarily Type I and III Collagen, which accumulate into scar tissue bands. Over time, these scars encircle healthy hepatocytes, narrowing the hepatic sinusoids and obstructing nutritional blood flow. Consequently, the hepatic lobule structure is disrupted, leading to the formation of regenerative nodules and cirrhosis, resulting in a total loss of essential biochemical functions.
2.2. Hepatitis B and C Viruses
Hepatitis B virus (HBV) and Hepatitis C virus (HCV) are the two leading infectious agents causing chronic hepatitis on a global scale.
Hepatitis B is a DNA virus capable of integrating its genome into the host hepatocyte’s DNA, making complete viral eradication extremely difficult. Chronicity is typically established when the surface antigen HBsAg persists in the serum for more than six months.
Conversely, Hepatitis C is an RNA virus with a very high mutation rate, allowing it to easily evade immune recognition. Without intervention through modern antiviral therapies, approximately 80% of acute HCV infections progress to chronicity, significantly increasing the risk of hepatocellular carcinoma.
2.3. Metabolic Disorders and MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease)
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD), formerly known as NAFLD, is becoming a prevalent cause of chronic liver disease in modern society. The pathogenic mechanism is based on the “two-hit hypothesis”: The first hit is the excessive accumulation of triglycerides in hepatocytes due to insulin resistance and caloric excess. The second hit involves oxidative stress and inflammation triggered by the release of free fatty acids. When this condition progresses to Metabolic Dysfunction-Associated Steatohepatitis (MASH), hepatocytes undergo “ballooning” and apoptosis, stimulating fibrosis in a manner similar to viral hepatitis. The danger of MASLD lies in its ability to progress silently even when liver enzyme levels remain within normal limits.
2.4. Toxicology of Alcohol and Industrial Chemicals
Alcohol (ethanol) is a direct hepatotoxin when consumed in large quantities over a long period. Once in the body, ethanol is metabolized by the enzyme Alcohol Dehydrogenase into acetaldehyde, a highly toxic compound capable of generating free radicals that damage cell membranes and mitochondria. Acetaldehyde also disrupts protein synthesis and promotes fat accumulation in the hepatic parenchyma.
Besides alcohol, long-term exposure to industrial chemicals like carbon tetrachloride, or the misuse of medications such as high-dose paracetamol, can cause chronic liver injury through cumulative toxicity mechanisms. These injuries often begin with steatosis and focal inflammation, eventually spreading into fibrosis if the toxic agent is not removed.
3. Classification of Liver Fibrosis Stages via the Metavir System
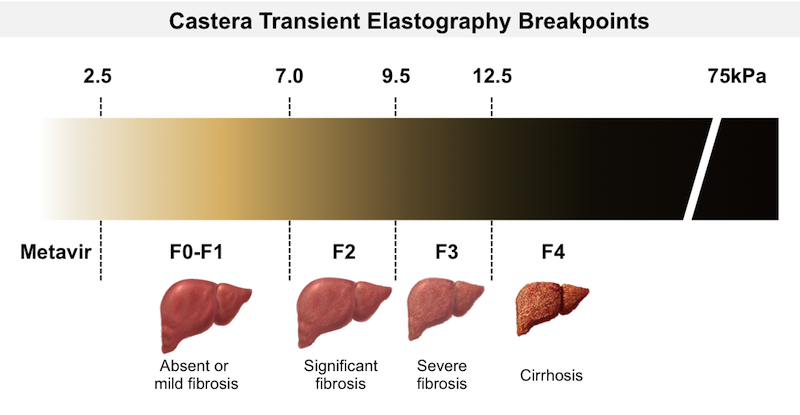
The Metavir system is the medical gold standard for classifying the severity of chronic liver disease based on histological changes.
- Stage F1 is characterized by mild fibrosis around the portal tracts without the formation of septa.
- Stage F2 assesses fibrosis that has spread, with the appearance of a few thin septa connecting the portal tracts.
- As the disease progresses to Stage F3, the fibrous bands thicken significantly, creating a phenomenon known as “bridging fibrosis,” which divides the liver parenchyma into distinct sections but has not yet completely disrupted the lobular structure.
- Stage F4 represents established cirrhosis, where fibrous bands encircle regenerative nodules, causing a total loss of lobular architecture and leading to portal hypertension, resulting in life-threatening complications.
4. Paraclinical Diagnostic Methods and Laboratory Indices
To accurately assess the severity of chronic liver disease, physicians utilize a multi-layered paraclinical testing system.
- Biochemical blood tests focus on two groups of indices: cellular injury markers (ALT, AST, GGT) and liver function markers (Albumin, Bilirubin, Prothrombin time). The ALT index is generally more sensitive to liver-specific injury, while an elevated AST/ALT ratio often suggests alcohol-induced damage.
- Beyond blood tests, Transient Elastography (Fibroscan) plays a pivotal role in quantifying the stiffness of the liver parenchyma, measured in kilopascals (kPa). Fibroscan results allow for the precise classification of patients into fibrosis stages from F0 (no fibrosis) to F4 (cirrhosis) without the need for invasive liver biopsy.
5. Antiviral Therapy and Supportive Pharmacological Strategies
Modern treatment of chronic liver disease prioritizes the elimination of the core pathogenic agent.
For chronic Hepatitis B, the primary goal is to inhibit viral replication through Nucleoside/Nucleotide Analogues such as Tenofovir Alafenamide (TAF) or Entecavir to prevent progression to cirrhosis and liver cancer.
For Hepatitis C, the advent of Direct-Acting Antivirals (DAAs) like Sofosbuvir and Velpatasvir has enabled a complete cure rate exceeding 95% after a 12-week regimen.
In addition to specific drugs, hepatoprotective agents such as Silymarin or Branched-Chain Amino Acids (BCAA) are considered to support parenchymal recovery and improve nutritional status in late-stage patients.
6. Nutritional and Lifestyle Management for Chronic Liver Patients
Nutritional management plays a role equivalent to pharmacological therapy in controlling chronic liver disease. Patient menus must be designed on the principle of providing sufficient energy while reducing the metabolic load on the liver.
Dividing food intake into 5-6 small meals per day helps maintain stable blood glucose levels and prevents muscle catabolism. Preference should be given to plant-based proteins or white proteins from poultry and fish to minimize ammonia formation. Strict control of salt intake below 2,000mg per day is mandatory for patients showing signs of fluid retention or ascites.
Additionally, moderate physical activity, such as walking or swimming, is encouraged to improve insulin sensitivity and reduce hepatic steatosis.
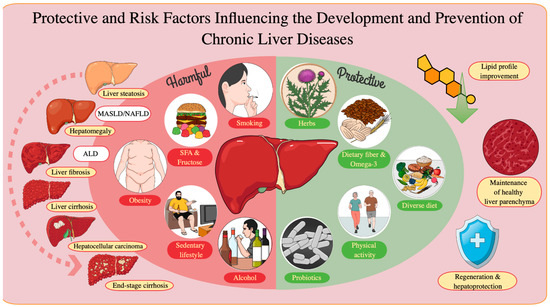
- Harmful Food Groups to Eliminate:
Patients must strictly abstain from alcohol as the toxin acetaldehyde directly destroys liver cells. Concurrently, canned foods and processed items containing high levels of nitrate salts should be removed to reduce the detoxification burden. It is essential to avoid raw seafood to prevent dangerous bacterial infections and to cut down on trans fats from fried foods to halt the spread of systemic inflammation.
- Supportive Food Groups for Recovery:
Priority should be given to cruciferous vegetables and turmeric containing curcumin to stimulate detoxifying enzymes and inhibit the formation of fibrotic scar tissue. Herbal teas such as artichoke and chamomile further assist in choleretic (bile-promoting) effects and improve digestion. However, these foods serve only as supportive measures and cannot replace specific medical treatments prescribed by a physician. Specialized nutritional regimens are developed based on the physiological changes of the liver through each fibrosis stage (F1 to F4), helping patients adjust their dietary intake appropriately for their current health status.
7. Complication Screening and Hepatocellular Carcinoma (HCC) Prevention
The most critical complication of chronic liver disease is the development of Hepatocellular Carcinoma (HCC). Continuous inflammation and cellular regeneration increase the probability of malignant genetic mutations. Consequently, all chronic liver disease patients, particularly those at fibrosis stage F3 and above, must be enrolled in a rigorous screening program. The standard protocol includes periodic abdominal ultrasounds and serum AFP (Alpha-fetoprotein) testing every six months. Detecting tumors early—when they are smaller than 2cm—allows for definitive interventions such as Radiofrequency Ablation (RFA), liver resection, or liver transplantation, thereby significantly extending patient survival and quality of life.
PARTNER SOLUTIONS FROM AUDACE PHARMA
Understanding the challenges of chronic liver disease and its dangerous complications, Audace Pharma has researched and developed a specialized product ecosystem to support liver cells. With a mission to protect comprehensive liver function and promote natural detoxification processes, we provide optimal solutions tailored to the specific needs of maintaining and restoring liver health for our customers.
For daily liver protection and enhancement needs, Atiso Pluss and Atiso are suitable choices to support liver detox. During phases requiring intensive liver function recovery or symptom relief from hepatitis, Orthymin Pluss, Nifamin Gold, and Livernifa serve as reliable companions to strengthen liver health.
The journey to control chronic liver disease is one of perseverance, and Audace Pharma is proud to empower you with professional, standard medical solutions. Let us help you build a solid protective barrier for your liver starting today. Do not hesitate to contact Audace Pharma to co-create sustainable liver protection and healthcare solutions.